【筋萎縮性側索硬化症】きんいしゅくせいそくさくこうかしょうamyotrophic lateral sclerosis〈ALS〉
中年以降に発症し,筋萎縮と線維束攣縮を主徴とする原因不明の疾患で,男性に多くみられる.病理所見は, 脊髄前角細胞 および延髄運動核の変性と,錐体路の変性である.初発症状は主として手の脱力,手指の運動障害,および上肢の線維束攣縮であるが,発病部位により,上肢型,球型,下肢型,混合型に分けられる.上肢型では母指球,小指球の萎縮による猿手,骨間筋の萎縮による鷲手,さらには前腕(特に屈筋)の筋萎縮がみられる.球型においては舌の萎縮と線維束攣縮,舌の運動障害,口蓋咽頭筋の萎縮による言語障害,嚥下困難をみる.下肢型では前脛骨筋,腓骨筋の萎縮により尖足が起こる.いずれの型でも症状の進行とともに全身の筋群が侵される.上位運動ニューロン症状として痙性麻痺,深部反射亢進,病的反射がみられ,下顎反射,口とがらし反射もみられることがある.進行性の経過をとり,3〜4年で死の転帰をとることが多い13
錐体路障害
http://www.md.tsukuba.ac.jp/basic-med/molneurobiol/brain/kenkyu16n/kenkyu02.html
Chinese Acupuncture Formulas for Treating Amyotrophic Lateral Sclerosis (ALS)
http://damo-qigong.net/als.htm
Acupuncture Formula 1
Acupoints Arrays:
1Bai Hui, Pi Yu, Shen Yu, Ming Men, etc.
2Shan Zhong, Guan Yuan, Qi Hai, Xue Hai, etc.
3Da Zhui, Qu Chi, Wai Guan, He Gu, etc.
4Feng Chi, Shou Shan Li, Nei Guan, etc.
Acupuncture Manipulation:
Every time choose either one of array 1 and array 2. Retain the needle while applying moxibustion. When choosing array 3 and array 4 use burning-fire manipulation method. Extract needle when patients feel hot. Apply the treatment one time each day during the first month and one time every other day one month later.
Treatment Notes:
20 times constitute one treatment course. During the treament, plum blossom needle should be used to slightly puncture place near neck, two sides of spine and atrophy areas. Stop the puncture when slight amount of blood issues. Partial massage are recommended in the same time.
Recording of Two Successful Cases:
Case 1. Male, aged 28. With ALS for 5 months without any improvement with normal treatment prescribed by western doctors. Then choose the acupuncture treatment above mentioned. After 120 days of treatment, all normal function of body trunk and four limbs is recovered. No recurrence during late days.
Case 2: Female, aged 41. With ALS for 1 year. No any improvement. Then received the acupuncture treatment above mentioned. Gained complete recovery after 5 monthes of consecutive treatment. No recurrence for the succeeding 4 years.
TREATMENT OF ALS WITH CHINESE MEDICINE
by Subhuti Dharmananda, Ph.D., Director, Institute for Traditional Medicine, Portland, Oregon
http://www.itmonline.org/arts/als.htm
Note: This article first appeared in March 1999, but additional information has been gained since then, particularly about the treatment method of Cheng Yongde, who specializes in treating ALS in China. In addition, drug therapies that had looked promising just a few years ago have turned out to be disappointing, making use of Chinese medicine of continued special interest.
BACKGROUND
ALS (amyotrophic lateral sclerosis) was first identified about 130 years ago. During the past 60 years it has been called Lou Gehrig's disease, named for the most famous of its victims (1903-1941), who had been a popular and vigorous baseball player until the disease struck. However, as memory of his life fades, the term ALS has become the preferred designation. This is a rare disease: in the U.S. it affects about 1-2 persons per 100,000 each year, with a cumulative total of about 25,000-30,000 living with the disease at any one time. It most often occurs in persons over 50 years of age (rarely before age 40), with more men than women affected. It is a degenerative disorder of the central nervous system that leads to weakening and wasting of the muscles. Depending upon which neurons are first affected, the disease will manifest differently among individuals, but eventually all four limbs become involved and there may be considerable cramping and stiffness that develops with the partial loss of nervous control over the muscles. A normal course of disease progression is to reach the point that respiration is affected within 5 years after the initial symptoms and diagnosis, causing death. There is about a 5% rate of survival past 12 years, and some people live more than 20 years, while others have rapid disease progression within just 2 years.
Riluzole was the first drug for ALS approved by the U.S. FDA. The drug inhibits glutamate release; glutamate is one of the major neurotransmitters and is an essential part of nervous system function. Excess levels of this amino acid are thought to be involved in ALS and some other neurological diseases, by causing nerve damage and death. Riluzole is far from an ideal therapy: it can have side effects (nausea, vomiting, or worsening of disease condition), it is quite expensive, and the survival effects are an average 2-3 month extension in life span. New drugs have been disappointing. For example, Myotrophin (insulin-like growth factor-I) had been used as an off-label application for ALS since 1991, apparently slowing the progression of muscle deterioration. Submitted for drug approval for ALS treatment five years ago, the FDA delayed granting approval because it did not have adequate evidence of efficacy and this drug appears to be out of further development for ALS, having displayed only modest results at best. Another example is BDNF (brain-derived neurotrophic factor), which appeared to slow the deterioration in breathing capacity, but further tests failed to confirm the result and research on it has been discontinued.
A growing body of research suggests that ALS, especially the hereditary type that appears at younger age, is associated with a defect in the enzyme called superoxide dysmutase (SOD), an antioxidant system, in which the SOD produced by the body changes from an antioxidant (that is protective to nerves) to a pro-oxidant that damages the nerves. Thus, antioxidant therapies might help slow progression of the disease, at least in individuals with this genetic defect. The possibility of beneficial effects from antioxidants has been proposed, but has not been confirmed. Indeed, many people with ALS turn to taking nutritional supplements rich in antioxidants but do not report significant improvements; formal studies have yet to be undertaken.
Due to the limited impact of readily available therapies, patients and their families may opt to seek out Oriental medical assistance, which is becoming more accessible every year as the number of practitioners grows (now at about 15,000 in the U.S.). Practitioner experience with ALS, due to the rareness of the disease, has been limited; fortunately, there is some information from China available to help guide treatment strategies.
ACUPUNCTURE
Acupuncture is thought to influence physiological functions via the nervous system, and especially by promoting blood circulation (see: Introduction to acupuncture). Nervous system disorders, including various paralytic diseases, such as stroke, traumatic paraplegia, and progressive myodystrophies, are treated by acupuncture in China. It is thought that promoting the microcirculation (capillary bed circulation) to the spinal cord can enhance the natural regenerative capabilities that exist. From the traditional medicine point of view, acupuncture can open the blocked meridians, including the one running through the spinal column known as the dumai or governing vessel (du = govern, supervise, direct; mai = channel, vessel, meridian). Whether neurons are damaged by physical trauma, blocked circulation of blood (as occurs in stroke), or by biochemical processes (e.g., oxidation reactions, excess glutamate), the principle of treatment via acupuncture remains the same. Two techniques are especially relevant to central nervous system diseases: scalp acupuncture and spinal acupuncture. Both involve treatments on or along side the governing vessel, which runs up the spine to the head, running over the center of the scalp (see Figure 1).
Scalp acupuncture (see: Synopsis of scalp acupuncture) is applied in the treatment of all neurological disorders. Most experience with this technique has been in treatment of stroke, but scalp acupuncture has shown some promise in treating degenerative neurological diseases as well. Zhu's Acupuncture Medical and Neurology Clinic in San Jose, California (www.scalpacupuncture.org), headed by Zhu Mingqing, provides scalp acupuncture treatments. Many acupuncturists in the U.S. have learned this method of treatment and can administer it closer to the home of the person with ALS, who will need treatment regularly for many months. The scalp acupuncture technique is best applied while movement is still close to normal, as the effects are most dramatic when the person moves of the affected body parts while the scalp needles are being manipulated. While there are several zones for treatment on the scalp, a major focal point of this acupuncture technique is threading needles along the scalp on either side of the Governing Vessel at the top of the head near the point baihui (GV-20).
For spinal acupuncture, two doctors have given some detailed recommendations: Wang Leting (1894-1990), whose method is described in the book Golden Needle Wang Leting (1) and Cheng Yongde, a specialist in encephalatrophy, Parkinson's disease, and ALS, currently working at the Municipal Hospital of TCM of Haimen (near Shanghai) in Jiangsu Province. Cheng published an article on treating 46 patients with ALS in a 1998 issue of the Shanghai Journal of Acupuncture and Moxibustion, with a shortened version published in the English-language edition of that journal. An extended version of the article was published in the Zhejiang Journal of Integrating Traditional Chinese Medicine and Western Medicine in 1999.
THE METHOD OF WANG LETING
Spinal treatment focuses on points of the governing vessel on the back, mainly from fengfu (GV-16), a point on the neck about 1 inch into the hairline, down the spine to yaoyangguan (GV-3), at the lower lumbar region of the spine (between L4 and L5 of the lumbar vertebrae). Fengfu is the point at which the governing vessel is said to enter the brain.
Wang Leting performed acupuncture in many cases of stroke and paraplegia utilizing these spinal points. His work on paraplegia is relevant to ALS, because the basis for the treatment is not dependent on the precise cause of the disorder, but, rather, its location of the pathology in the spine. His main methods for treating paralytic disorders is to administer acupuncture to a group of points on the governing vessel as well as a group of the Hua Tuo points on either side. The set of points he recommends for treating the governing vessel includes baihui (GV-20) at the top of the head and changqiang (GV-1) just below the tip of the coccyx, and then this series along the spine:
fengfu (GV-16)
dazhui (GV-14)
taodao (GV-13)
shenzhu (GV-12)
shendao (GV-11)
zhiyang (GV-9)
jinsuo (GV-8)
jizhong (GV-6)
xuanshu (GV-5)
mingmen (GV-4)
yaoyangguan (GV-3)
This group of 13 points constitutes one treatment, which can be treated along with and alternated with other point sets that are deemed necessary, especially the Hua Tuo points. Administering acupuncture each day, alternating treatment between two sets of points so that the treatment on two consecutive days is not a repetition, is standard practice in China for treating serious diseases.
Wang preferred treating the Hua Tuo points slightly closer to the spine than their usual location, namely, at 0.3 cun rather than 0.5 cun lateral to the spine (see: Hua Tuo). He would treat every other vertebral site, starting with the lower edge of the second thoracic vertebra down to the 4th lumbar vertebra, a total of 16 points treated bilaterally. This needling on both sides of the governing vessel is supposed to have the effect of promoting qi circulation that crosses the damaged area. The same basic tactic was used in a recent clinical report on treating traumatic paraplegia (4), in which the main points chosen were the Hua Tuo points and the bladder channel points that lie lateral to them, just a little further from the spine (1.5 cun), on the back.
THE METHOD OF CHENG YONGDE
Cheng Yongde noted that in the past Chinese physicians mainly relied on the ancient doctrine of the Niejing Suwen (ca. 100 A.D.) in treating diseases where the muscles atrophy. The basic approach they take when encountering a disease that causes the muscles to weaken and atrophy is to direct treatment at enhancing the function of the stomach/spleen system, rooted in the concept that the spleen governs the muscles. By treating the associated meridians (e.g., yangming meridian), the muscles would be nourished and invigorated. Cheng believes, instead, that ALS is due to a blockage of the governing vessel, leaving it unable to regulate the qi and blood flowing to the viscera; then, the limbs are not adequately nourished by the flow of qi and blood. Therefore, using acupuncture to unblock the governing vessel is the key to therapy. This is his 1999 report (edited slightly).
ALS is an illness of the motor neurons. The pathological alteration affects mainly the anterior kerato-cell of the spinal cord, motor neural kernel of the lower brain stem, and the motor cortex corpus-vertebral cell of the brain. As a result of a degenerative change of the myelolateral cord, the spinal cord becomes atrophic and smaller; further, degenerative damage of the anterior kerato-cell and the motor neural kernel of the medulla oblongata and pons varolii occurs. The muscles then atrophy due to lack of control by the nerves that influence their function. Traditional Chinese medicine ascribes it to the category of wasting syndromes (weizheng). The author had treated total of 46 ALS patients from 1980 to 1996, and this is the clinical report.
The group of patients comprised 27 males and 19 females (3 patients were aged 21-30 years, 4 aged 31-40, 10 aged 41-50, 25 aged 51-60, and 4 aged over 61). As judged by initial symptoms, two patients had the bulbar type, 8 had the cervical medulla type, 13 had the lumbar medulla type, and 23 had the mixed type of ALS. Pathogenesis after initial appearance of the disease shows cryptic and gradual progression, with clinical symptoms associated with the lesions of either the upper and lower motor neurons or both; the electromyogram displayed lesions of the motor neuron. The indicators for this group of patients were in accord with the diagnostic criteria for ALS, so the diagnosis was clear and definite.
Acupuncture was performed in a manner unique to each individual but the acupoints were mainly fengfu (GV-16), dazhui (GV-14), and the Hua Tuo points, used together with both local and distal points (mainly jing points) on the meridians traversing the muscular atrophic part. The acupoints were arranged in groups, using one set one day, and another set the next day, and then repeating this basic treatment. For Hua Tuo points, about eight points would be needled bilaterally along the area of the spine affected by the disease. Needle stimulation was adjusted to apply tonification or draining with the needle directed along or against the direction of the meridians, the technique selected to enhance and normalize the flow of meridian qi. The first course of treatment for each patient was 1-3 months, needling once per day or every other day; this was followed by the second and the third course administered according to the patient needs (in terms of frequency of treatment and overall number of courses).
Patients also took the formula Sanqi Fuwei Ruansuo Wan (Atrophy Restoring and Cord Softening Pill) designed by the author, comprised of tien-chi ginseng, deer horn glue, and processed pangolin scale as the main ingredients. The herbs are ground to powder, made into pills and taken 10g a time, 3 times a day, for a duration of 6-24 months.
After applying acupuncture to open the governor vessel, and using the herb pill to tonify and disperse slowly, physical exercise therapy was employed to promote restoration of physical function. Patients were trained to undertake an improved Ba Duan Jin Qi Gong (literally, eight pieces of brocade exercises) with emphasis on concentrating one's mind at the dantian (just below the umbilicus). These physical exercises, which included having the patients make some wide circular motions with the arms and torso and performing some deep breathing exercises, could promote restoration of the atrophic muscles and sustain normal functions of the non-atrophic muscles.
The results of therapy were classified into four categories: clinical remission, where atrophic muscles were largely restored, the patient then being able to manage daily activities and take place in social activities, or being able to survive with the disease more than ten years after diagnosis; markedly effective, where the ability of managing daily activities was enhanced somewhat, or being able to survive more than five years after diagnosis; fairly effective, muscular atrophy slows down, with survival over three years; ineffective, symptoms do not significantly improve with survival less than three years. Of the 46 patients, 6 appeared to have clinical remission; for 11 the treatment was markedly effective; for 24 it was fairly effective, and for 5 it was ineffective (the patients died within a few months time).
ALS is a recalcitrant atrophic disease. In ancient times, many practitioners treated the atrophic syndrome from the point of view that since the spleen governs the muscles, "choose the yangming meridian alone" as the therapeutic principle, originally described in the Neijing where it was taught that deficiency in this meridian yielded flaccid paralysis. This viewpoint emphasizes only the nutritional role of the spleen on the muscles (extracting the essence of food and water), but neglects modulating the distribution of the vital essence to the governing vessel. The governing vessel is an extra meridian, independent of the visceral main meridians. So, to treat certain atrophic syndromes, especially ALS, by the spleen tonification method seems quite hopeless. Planning the treatment for atrophy through the governing vessel goes beyond the limited framework of "choose the yangming meridian alone" and reliance on the doctrine that "the spleen governs the muscles." It has opened up a new way for the treatment of ALS, consistent with our modern knowledge that the disease affects the spinal cord first, not the muscles first.
The limbs are the root of all yang, which are in close relationship with governing vessel being the sea of yang channels running through the vertebra to govern all meridians. If the limbs are not regulated through the governing vessel, the visceral qi and blood are unable to nourish the limbs through the main meridians. In the case where the governing vessel becomes gradually blocked, its ability to control the limbs would be limited progressively, and the muscles of the limbs become withered due to insufficient nourishment by the visceral qi and blood. Eventually modulation by the governing vessel is abolished, the limbs, and even all the other muscles of the body, become atrophied. So, the treatment of ALS is based upon opening the governing vessel.
The governing vessel is nourished by the meridian qi of the central viscera. If the viscera become weakened, the essence of the main meridians becomes deficient and is unable to nourish the governing vessel sufficiently, and this process will result in debility. It is a well-known doctrine that "the site with extreme deficiency is the usual place of invading pathogens." The external pathogens include the six excesses (wind, cold, summer-heat, dampness, dryness, and fire) that exploit bodily weaknesses to invade into the governing vessel and are retained, unable to leave. This retention of pathologic influence as a result of weakness of the governing vessel induces accumulation of phlegm and dampness, stasis of qi and blood, and toxicity and heat lingering for a long time. In such case, there is a deficiency of the normal qi and excess of the pathogenic factors (external evils). By this mechanism, the governing vessel becomes blocked; it then loses its ability to regulate the muscles, thus resulting in amyotrophy.
"Treatment of diseases ought to be aimed at their roots." One must first dredge the governing vessel, relying upon this meridian to regulate and improve the nutrition of the muscles. This approach should effectively limit the development of sclerema of the lateral cord, to limit, halt or even reverse the progressive amyotrophy in this disease.
The principal therapeutic means employed in these cases was acupuncture that was focused on dredging the governing vessel. The major acupoints were needled very deeply, that being a key to dredging the governing channel. The author needled the fengfu (GV-16) point slowly and deeply, to a depth of up to 10 cm (aimed downward to pass along the spinal cord) more than thousand times without having any accidents. However, the acupuncture practitioner must pay much attention to the details of the needling [see note below]. Dazhui (GV-14) was also needled slowly and deeply. The administration of herb pills and use of physical exercises should adhere to the principle of getting the governing vessel strong and being dredged. The three therapeutic measures-acupuncture, herbs, and exercises-should be carried out successively to get the desired results, though whether the latter two means are essential for getting better results with ALS is suggested but needs further clarification.
Noted by the journal editor: needling of the fengfu (GV-16) acupoint to a depth of around 10 cm (more than 3 cun) was solely used in clinical practice by the author of this article and is not common practice. The editors consider that needling at the fengfu point with an excessive depth might put the patient at the great risk; if readers want to adopt this acupuncture therapeutic method, they must contact the author first before attempting to employ this needling maneuver in clinical practice. Usual needling of fengfu is to a depth of 0.5-0.8 cun, though points along the spinal column are sometimes needled to a depth of 1.0-1.5 cun (see Figure 2 for a similar type of deep needling at GV-15); even at this depth, special training in needed and precautions must be taken.
In the book Acupuncture Treatment for Paralysis (4), the therapy for paraplegia due to spinal injury is somewhat similar to that recommended by Wang Leting and Cheng Yongde. The authors recommend needling the governing vessel just above and just below the site of injury and needling the Hua Tuo points on both sides. Adjunctive points are treated for the specific areas or body functions affected, or for the general purpose of promoting the production and circulation of qi and blood.
HERBS
Herbal therapies for ALS are aimed at nourishing the kidney to benefit the marrow and spinal cord, and at vitalizing blood to soften the sclerosis and to invigorate the circulation to the affected muscles. The traditional formula most often mentioned for treatment of wasting syndrome is Huqian Wan (Hidden Tiger Pill), which is sometimes modified by adding additional tonic herbs (see: Chinese herbal treatment of multiple sclerosis and other flaccidity syndromes). A key herb in this formula is tortoise shell, which is used for flaccidity and debility, especially of the lower limbs. However, the basis for the design of Huqian Wan is the concept that a heat-type disease damages the yin fluid, leading to the atrophy of muscles. For this reason, Huqian Wan contains rehmannia, tortoise shell, and peony to nourish and retain the yin essence, and anemarrhena and phellodendron to quell the deficiency fire of the kidney that threatens the remaining yin. Although this mechanism may apply to some cases of ALS, there is no clear evidence that a heat-type syndrome precedes its development or that yin deficiency heat dominates the syndrome. Thus, treating flaccidity as if it is due to yin deficiency with heat may-like the idea of treating it as if it is due to spleen deficiency, with failure to nourish and generate the muscles-be inadequate for diseases of the spinal cord. So, other ideas must also be considered.
Regeneration of the damaged nerves and bones is often attempted with deer antler or its gelatin, which is considered one of the main herbs for tonifying the governing vessel. Tortoise shell and antler gelatin were used in a case study involving ALS. The formula, provided to a small number of patients, had deer antler gelatin, tortoise shell, rehmannia, tiger bone, dipsacus, cuscuta, eucommia, atractylodes, licorice, (with astragalus added for a later prescription), eucommia, achyranthes, tang-kuei, peony, phellodendron, anemarrhena, and citrus (5). As described in the case of paraplegia due to injury (6): "The governing vessel travels along the back and is in charge of the yang qi of the whole body. Damages in the governing vessel cause yang deficiency." For this reason, many modern formulas for flaccidity and wasting, such as this one, also include yang tonic herbs, such as dipsacus, deer antler, cuscuta, and eucommia.
A formula Yisui Tang (Boost the Marrow Decoction) used for progressive spinal myodystrophies, including ALS, is similarly formulated: it is made with tortoise shell, deer antler gelatin, rehmannia, dipsacus, cuscuta, atractylodes, licorice, astragalus, psoralea, cibotium, achyranthes, tang-kuei, peony, millettia, phellodendron, and anemarrhena. This combination, given as a decoction with 9-15 grams of each ingredient (except only 5 grams each of phellodendron and anemarrhena), was used to treat 110 patients, of which 30 were diagnosed as having ALS (7).
As pills, the herbs are taken in doses of 3-9 grams each time, 2-3 times daily (total dose 9-18 grams per day), while the decoctions are taken in high dosage of 150-180 grams per day. The clinical reports in which the herbs were utilized claimed benefits for ALS patients, though the small number of patients involved makes it somewhat difficult to interpret the results.
A disadvantage of herb-only protocols in the West is that it is too easy for a patient to become discouraged if there are a few difficult days and then stop taking the herbs. This easy discontinuance of therapy occurs especially because herbal therapy is not a routine practice here, so there is little support for continuing treatment. With regular office visits for acupuncture, it is easier to adjust the herbal treatment as needed and to give immediate symptom relief with the acupuncture while, at the same time, encouraging compliance with the herbal protocol.
REFERENCES
Yu Huichan and Han Furu, Golden Needle Wang Leting, 1996 Blue Poppy Press, Boulder, CO.
Cheng Yongde, Formulating a therapeutic program with the governing vessel in treating 46 cases of ALS, Shanghai Journal of Acupuncture and Moxibustion 1998; 17(5): 43. (in Chinese)
Cheng Yongde, Clinical observation on 46 cases of amyotrophic laterial cord sclerema (ALS) in consideration of the treatment principle breaking through the Dumai (GV), Zhejiang Journal of Integrating Traditional Chinese Medicine and Western Medicine 1999; 9(1): 16-17. (in Chinese)
Kong Yaoqi, Ren Xingsheng, and Lu Shaokang, Acupuncture Treatment for Paralysis, 1996 Science Press, Beijing.
Zhang Jianguo, Chronic progressive spinal lateral sclerosis, Journal of the College of Traditional Chinese Medicine 1985 (4): 66-67.
Gao Xipeng, et al., Acupuncture treatment of complete traumatic paraplegia, Journal of Traditional Chinese Medicine 1996; 16(2): 134-137.
Fruehauf H, Treatment of Difficult and Recalcitrant Diseases with Chinese Herbs, 1997 ITM, Portland, OR.
APPENDIX. ITM FORMULARY
A version of Huqian Wan is produced as Tortoise Shell Tablets (Seven Forests); Antler 8 (Seven Forests) provides a significant dose of deer antler, and additional deer antler is available in White Tiger Pantosterone. Tien-chi Ginseng (Pine Mountain) is available as a single herb tablet, and herbs for tonifying the governing vessel are included as major ingredients of Eucommia 18 (Seven Forests). Antioxidants are obtained with the White Tiger formulas Quercenol, Cartaequin, Calmagnium, and Alpha-Curcumone.
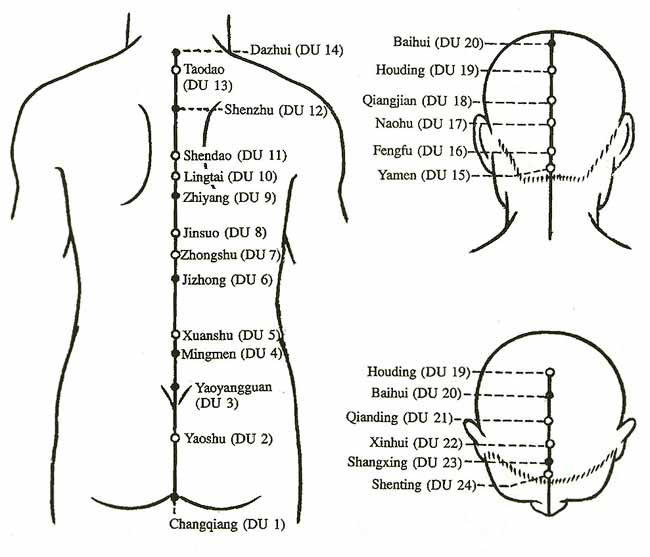
Figure 1: Points on the Governing Vessel (Du Mai). The points are labeled either DU, as in this illustration, or GV, as in the text.
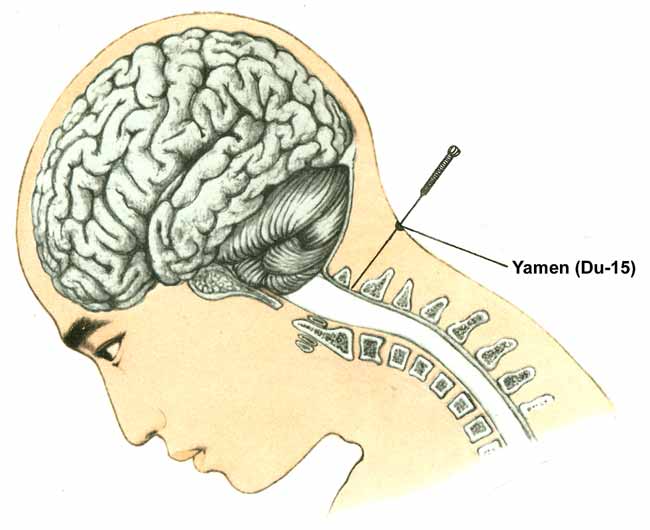
Figure 2: Location for needling yamen, a point on the governing vessel midway between fengfu (DU-16) above it and dazhui (DU-14) below it. This illustration shows the maximum depth of needling and the position of the patient (sitting up, with head bent forward) commonly used during this treatment. Deeper needling is done at an angle, so that the needle does not penetrate the spinal cord. Practitioners should avoid deep needling of these points unless adequate training has been undertaken.
Electroacupuncture reduces neuroinflammatory responses in symptomatic amyotrophic lateral sclerosis model.
Yang EJ, Jiang JH, Lee SM, Hwang HS, Lee MS, Choi SM.
J Neuroimmunol. 2010 Jun;223(1-2):84-91. Epub 2010 May 10.
Department of Standard Research, Korea Institute of Oriental Medicine, Yuseong-gu, Daejeon, Republic of Korea.
http://www.ncbi.nlm.nih.gov/pubmed/20460191
Abstract
Amyotrophic lateral sclerosis (ALS) is a paralyzing disorder that is characterized by the progressive degeneration and death of motor neurons. Acupuncture or electroacupuncture (EA) has been used for the treatment of various conditions including osteoarthritis, asthma, and other types of chronic pain conditions. It has been hypothesized that acupuncture exerts anti-inflammatory and anti-nociceptive effects on inflammatory reactions processes. The purpose of this study was to determine whether acupuncture at a specific acupoint could produce anti-inflammatory responses and suppress motor neuron loss in the hG93ASOD1 mouse, commonly used as a model for inherited ALS. We delivered EA at the Zusanli (ST36) acupuncture point in the symptomatic hSOD1G93A animal model. The EA-treated mutant hSOD1 transgenic mice showed decreases in microglial cell activity and TNF-alpha expression in the spinal cord and brain stem. Furthermore, EA significantly improved motor activity compared to the control group and reduced neuronal cell loss in hSOD1G93A mice. Our research suggests a potential functional link between EA therapy and anti-neuroinflammatory response in an ALS animal model.
Copyright 2010 Elsevier B.V. All rights reserved.
PMID: 20460191 [PubMed - indexed for MEDLINE]